Relieved with nitro (35% with ACS, 41% without ACS)
Relieved with GI antacids like "pink lady"
Features not characteristic
Pleuritic 13%
Sharp or knife-lung in respiration (22%)
Midline or lower abdomen
Pain localized with 1 finger
Pain reproduced with arm movement or palpation (7%) (high NPV)
Brief episodes (few seconds or less)
Maximal at onset
NOTE: Historic characteristics increase/decrease likelihood that chest pain is ischemic, but none rule it out
Diagnostic Tests
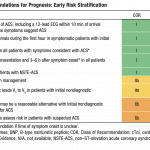
12-lead ECG (Repeat if diagnosis is unclear) – at 15-30min intervals if high risk of suspicion
NSTEMI ECG could have persistent or transient ST depression, transient ST elevation, T-wave inversion, flat T waves, pseudo-normalization of T waves or it can be normal.
Cardiac Biomarkers
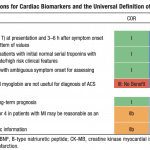
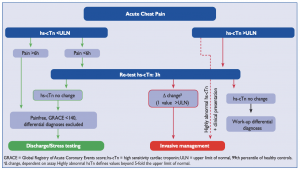
Serial cardiac Troponin I or T at presentation and at 3-6hrs after SYMPTOM onset (AHA 2014) (ESC 2015 promotes 0/3hr from PRESENTATION; 0/1hr algorithms validated for some assays)
Additional troponin level can be obtained beyond 6 hours in patients with normal serial troponin levels if there is intermediate/high suspicion for ACS
High-sensitivity cTn rises within 1h, and can remain elevated for days/weeks.
Repeating troponin levels until they "peak" is not recommended and is not helpful. Checking the troponin more than 3 times is generally a poor use of resources.
However, additional biomarker measurement on day 3 or 4 can help prognosticate and determine infarct size (particularly CK)
NOTE: If your institution has Troponin T, assume it is "high-sensitivity." Troponin I has many assays, but most modern institutions use high-sensitivity Troponin I assays.
CK-MB
Released from myocardium much more rapidly, and "peaks" earlier than troponin.
Generally less sensitive than troponin, and less specific for myocardium
May correlate better to infarct size
May be helpful if you suspect patient is having a second ACS event, and troponin is still rising from the initial event
UA/NSTEMI Recommendations (AHA 2014)
Biomarker Recommendations (AHA 2014)
Approach to Chest Pain & Classification
Categories of Ischemic Chest Pain
Initial assessment of patients should:
Establish likelihood that chest pain is due to myocardial ischemia
Rule out other main causes of chest pain (aortic dissection, PE, pericarditis)
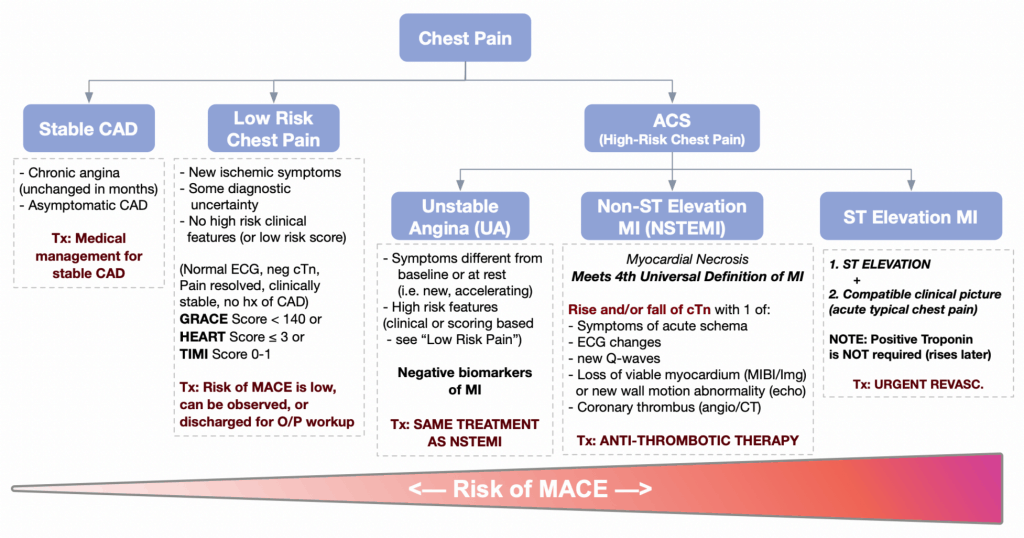
Classify patients into the following categories:
STEMI, NSTEMI, unstable angina, low risk chest pain, and stable angina (see below)
Risk stratify the patient into "high risk of MACE" or "low risk of MACE" clinically
(NOTE: Does not apply to STEMI, which is always considered high risk)
Categories of patients presenting with ischemic chest pain:
STEMI – ST elevations with compatible clinical picture
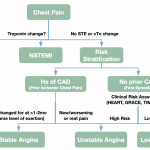
NSTEMI – Rise and fall of cardiac biomarkers, which meets the Universal Definition of MI
Unstable Angina – New/rest/changing pain without cTn or ECG changes, but "HighRisk of MACE" (see below)
Generally benefit from admission and aggressive antithrombotic therapy; so treated the same as NSTEMI
Low Risk Chest Pain – New/rest/changing pain without cTn or ECG changes, but "Low Risk of MACE" (see below)
Generally benefit less from aggressive/invasive therapy. These patients can be treated with observation/outpatient management with ASA, nitro spray, activity precautions until further assessment is done
Stable Angina– Predictable retrosternal chest pressure worse on exertion/stress, better with rest/nitroglycerin. To be "stable," the pain must remain unchanged for at least 2 months.
NOTE: Patients with stable angina who have a change in the pain, such as worsening pain, brought on by less exertion, or pain at rest, should be risk stratified to unstable angina or low risk chest pain.
How do I know if my patient is "Low Risk of MACE" or "High Risk of MACE"? You must risk stratify them using one or more of the tools below:
Clinical picture(Normal ECG? resolution of chest pain? history of CAD? clinically stable?)
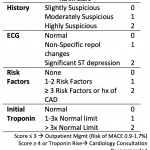
HEART Score ≤ 3(New, well-validated, best correlates to 30d risk of MACE)
GRACE Score < 140(Endorsed by ESC Guidelines 2015, better c-statistic than TIMI score)
TIMI Score 0-1(Endorsed by AHA Guidelines 2014)
Stress Test (if able to obtain quickly)
NOTE: You should know the main categories of the HEART and GRACE scores to quickly risk stratify ACS patients clinically.
Approach to classifying chest pain in ER
HEART Score
GRACE Score (Adapted from Emad Abu-Assi et al 2010)
TIMI Score Components (Adapted from MDCalc)
Low Risk Chest Pain
No ST elevation + no cTn change + and deemed low risk through:
There is often diagnostic uncertainty as to the cause of chest pain
Risk of MACE is low, and after a period of observation (+/- 3rd cTn) these patients can often be managed in an outpatient setting with close follow-up:
ASA is recommended (Class IIB)
Risk factor modification
These patients benefit less from intensive anti-thrombotic therapy and revascularization.
Those who may benefit may be further selected with non-invasive risk stratification:
Generally considered to be an ACS (plaque rupture/instability), but amount or duration of ischemia is insufficient to cause myocardial infarction and elevate biomarkers.
Classic patient is someone with on/off chest pain that lasts <30-60min at a time.
To call UA, there should NOT be any rise/fall of cTn on serial testing, and there should be concern that the chest pain is "high risk" based on clinical assessment or scoring (HEART, GRACE or TIMI)
Management
Hospital admission with medical management is the SAME as NSTEMI to treat plaque rupture/instability (see below)
Compared with NSTEMI, there is less benefit with revascularization
Patients can be selected for further risk stratification to determine if they will benefit from revascularization through non-invasive tests (i.e. exercise ECG, stress echo, MIBI, Cardiac CT
Based on numerous factors, some clinicians may prefer invasive coronary angiography
Practical Tip: New studies indicate that in the modern era of high-sensitivity cTn, negative cTn is excellent at predicting low risk of MACE. Overall the diagnosis rate of UA is declining. Most of the cTn-negative patients are classified as "Low Risk Chest Pain."
NSTEMI
Must qualify as "Myocardial Infarction (MI)", which is based on the Universal Definition of MI
Patients with NSTEMI should generally be admitted to hospital and treated with antithrombotic therapy (below)
4TH UNIVERSAL DEFINITION OF MI
Rise and/or fall of cTn with 1 of:
Symptoms of acute ischemia
ECG Changes
New Q-waves
Loss of viable myocardium (MIBI/Imaging) or new wall motion abnormality on echo
Coronary thrombosis directly visualized by CT or angiography
Management: Symptom Management
Oxygen: Supplemental only if sat ≤ 90% (routine O2 = poor outcomes)
Nitrates:
Indications: Chest pain, HF, hypertension
Benefit: Symptoms only (no effect on MACE)
Doses/Options: Nitro spray 0.4mg q5min x3
If pain beyond 3 nitro sprays, start infusion
Infusion Dose: 20 mcg/min IV → increase by 20 mcg/min increments until pain is controlled (max 400 mcg/min)
If infusion is not desired or the patient has intermittent chest pain, a nitro patch can be considered (or a low dose infusion): 1.2 mg/hr patch is equivalent to 20 mcg/min infusion
Contraindications:
PDE Inhibitors: within 24 hours of sildenafil or vardenafil, or within 48 hours of tadalafil
Hypotension
NOTE: Chest pain refractory to antithrombotic therapy and nitrates is an indication for immediate invasive therapy.
Morphine:
Indications: Only if pain refractory to all anti-ischemic agents
Suggestion of harm – (i.e. interference with anti-platelet agents, risk of HF, etc.)
Management: Antithrombotic Therapy
Dual Antiplatelet Therapy
Indications: All post-MI patients
Benefit: CV mortality, recurrent MI, need for revasc, etc. (MACE)
Stop at revascularization, discharge or 48hrs (whichever comes first)
1st Line: Enoxaparin 1mg/kg SC q12h (OD dosing if CrCl < 30 mL/min)
Patients for non-invasive approach: ESSENCE Trial: superior to heparin for mortality (continue through hospitalization or until PCI performed).
Patients for invasive approach: Many interventional cardiologists recommend against enoxaparin if patient is undergoing invasive approach (SYNERGY Trial: comparable to UFH in efficacy in pts undergoing invasive approach, but increased risk bleeding)
2nd Line: Bivalirudin (expensive in Canada, generally used in patients with HIT)
PRACTICAL TIP:
If PCI is planned, guidelines recommend any of the three first line agents but UFH is often preferred. In modern studies, enoxaparin showed similar outcomes but increased in-hospital major bleeding (SYNERGY) and fondaparinux had increased catheter thrombosis during angiography requiring a bolus of heparin (OASIS-5). OASIS-5 results also suggest that patients at high risk of bleeding can be considered for fondaparinux.
If conservative/medical managementis planned guidelines prefer fondaparinux or enoxaparin over heparin due to improved outcomes/convenience and decreased bleeding (ESSENCE). Again, in patients at high risk of bleeding, fondaparinux is preferred (OASIS-5)
GPIIB/IIIA inhibitors– Only used by interventional cardiology for bailout situations / thrombotic complications.
Management: Adjunctive Therapies
See CardioGuide: Post-MI Care
Management: Revascularization
Guidelines
Unlike STEMI, the benefit of revascularization of UA/NSTEMI without "high-risk features" has been controversial.(See "Evidence for revascularization strategies" below.)
Physicians should select an approach based on risks/benefits, and patient/physician preference.
Available Approaches
Routine Invasive: Invasive diagnostic evaluation (angiogram) +/- PCI for ALL patients
Early Invasive Strategy -> within 24hrs
Delayed Invasive Strategy -> within 25-72hrs
Ischemia Guided Strategy: Medical management. Invasive intervention only if:
Failure of medical therapy (ongoing ischemic chest pain)
High prognostic risk (TIMI/GRACE)
High-risk non-invasive stress test
If reasonable, a non-invasive risk stratification test can be used to determine if the patient is "high/intermediate risk" and may benefit from invasive management (most commonly MIBI)
AHA 2014 & ESC 2015 (see strategies to the right)
Indications for Invasive Evaluation in UA/NSTEMI
Urgent / Immediate Invasive Strategy
Refractory angina
Hemodynamic or electrical instability
Early Invasive Strategy (within 24hrs)
AHA 2014: If elevated risk of clinical events (see table to the right)
ESC 2015: If troponin rise/fall
Ischemia Guided Strategy (Conservative)
AHA 2014: Stable patients – reasonable considering clinician and patient preference
(Review the ESC and AHA algorithms to the right)
AHA 2014 Selecting Revascularization Strategy
ESC 2015 Selecting Revascularization Strategy
Summary of Evidence
FRISC-IITrial (1999) – Intermediate to high risk patients (FRISC score)
Early invasive strategy >> Ischemia-Guided (fewer recurrent MI and improved long-term survival)
Very old trial – poor medical therapy available at that time.
Definition of MI had issues (i.e. Troponin often not used, peri-procedural MI missed)
TACTICS-TIMI 18Trial (2001) – pts with unstable angina and NSTEMI
Early Invasive >> Medical Management (only if TIMI > 2)
ICTUS Trial (2005) – Pts with elevated troponin.
Early invasive = Ischemia Guided
Most recent data with relatively modern medical therapy.
RITA-3 Trial (2002) – pts with non-ST-elevation ACS
Early Invasive >> Medical Management for "refractory angina", equal for death and MI
Meta-Analysis of 7 RCTs: (Bavry JACC 2006)
Early Invasive >> Med Mgmt for NSTEMI
Bottom Line:
Revascularization appears to consistently confer a benefit in reducing angina, and possibly mortality benefit ONLY in "high/intermediate risk" groups.
Overall, trials controversial due to non-standard risk-stratification methods and variable definitions of MI.
ESC 2015 guidelines recommend routine invasive management if there is a troponin change
AHA 2014 guidelines recommend either approach, leaning towards early invasive in patients with high or intermediate risk. (To estimate risk, use GRACE, TIMI, or table above)
References
Primary Author: Dr. Pavel Antiperovitch (MD, FRCPC, Cardiology Fellow)
Author/Reviewer: Dr. Atul Jaidka (MD, FRCPC, Cardiology Fellow)
Staff Reviewer: Dr. Terrance McPherson (MD, FRCPC[Cardiology])


0 Response to "Given No Extraneous Circumstances Eg St Elevation Mi Continued Bleeding a"
Post a Comment